The silent struggle of Long COVID patients in Nevada


This story originally appeared in the Sierra Nevada Ally and is being republished here as part of a content-sharing agreement. Read the original version here.
When Crystal, a Sparks resident, contracted COVID-19 in 2021, she lost her taste and smell for nine months. Just as her senses began to return, new complications emerged — fatigue, memory fog and a dramatic 85-pound weight loss.
Over the next several years, she cycled through doctors and nutritionists, tried smell training and searched for answers, only to be told by some physicians that her symptoms were "all in her head."
"I was put through many medication trials and also diagnosed with mental illnesses because of this, with some saying that it was just OCD or making it up for attention. That was the most painful thing to hear," Crystal recalls.
The toll on her physical and mental health has been profound. To this day, she still cannot eat and enjoy chocolate or drink a cup of coffee, and many fruits and vegetables taste different from what she remembers. She has been left to navigate years of insufficient treatment, natural remedies and isolation — while holding onto hope that her health, and her joy in food, will one day return.
Crystal has been diagnosed with Long COVID, also known as Post-COVID condition (PCC), and her case is far from unique. She is one of an estimated 65 million to 200 million people worldwide — including 3 million to 5 million adults in the United States — living with the long-term health consequences of COVID-19.
What is Long COVID?
Long COVID is a growing public health concern. Because its symptoms vary widely and often overlap with other illnesses, it is especially complex to diagnose and treat, leaving patients like Crystal without clear answers or treatment pathways.
Across the country, several states have established specialized clinics to address the condition, but Nevada has fewer options and additional challenges. The state already struggles with limited access to health care — workforce shortages stretch across nearly every type of health professional.
This combination of complex diagnosis, limited specialized clinics and systemic shortages leaves Nevadans such as Crystal without the care they need, adding to the public health concern of a silent crisis that strains health systems, national economies and individuals' lives.
Experts around the world don't yet have all the answers. The World Health Organization defines Long COVID as the "continuation or development of new symptoms three months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least two months with no alternative explanation." It is characterized by multisystemic symptoms that affect daily life, ranging from neurological to cardiovascular to mental health conditions.
It is not yet known why some people experience Long COVID, and no preexisting conditions have been identified as predictors. What is clear is that it can affect anyone who has had COVID-19, regardless of the severity of their illness, age, race or ethnicity, sex, or baseline health status. The Centers for Disease Control and Prevention (CDC) lists common symptoms such as shortness of breath, persistent cough, fatigue, difficulty thinking or concentrating, rapid heartbeat or palpitations, joint and muscle pain, chest or stomach pain, changes in taste or smell, sleep problems, fever, rashes and even menstrual cycle changes.
In more severe cases, Long COVID can also involve autoimmune-related conditions and multiple organ complications.
Health care gaps in urban and rural Nevada
Other states, such as California, Florida, Illinois, Massachusetts, New York and Ohio, have established Long COVID/post-COVID clinics. In Nevada, however, options remain limited: in Southern Nevada, patients can turn to the UMC Southern Nevada Quick Care COVID Recovery Clinic, while in Northern Nevada the closest option is the Renown Health Pulmonary Rehabilitation Center.
Nevada lacks a robust health system and infrastructure to consistently provide quality health care and respond to public health challenges — an issue that was exacerbated by the COVID-19 pandemic. According to the Silver State Health Improvement Plan 2023–2028 by the Nevada Division of Public and Behavioral Health, the pandemic "highlighted and intensified population-level health inequities in access to and quality of care, as well as disparities in health outcomes that have existed for years."
The report underscores that all of Nevada's 17 counties have some form of shortage designation, with 70 percent of Nevada's population living in a primary care shortage area. These gaps are most severe in rural and frontier regions, where residents face higher costs, long travel distances and fewer providers.
"To meet national provider-to-patient averages, Nevada would need an additional 255 family medicine physicians, 626 nurse practitioners and 3,162 registered nurses, among other professionals," the report says.
In rural communities such as Yerington, specialty care exists but is stretched thin, explained Lea Pope, rural health education coordinator with the UNR School of Medicine.
"The biggest barrier is either access to specialists or transportation. It's scary for a patient to wait three or four months to get answers, so they end up going to Carson or Reno," Pope said.

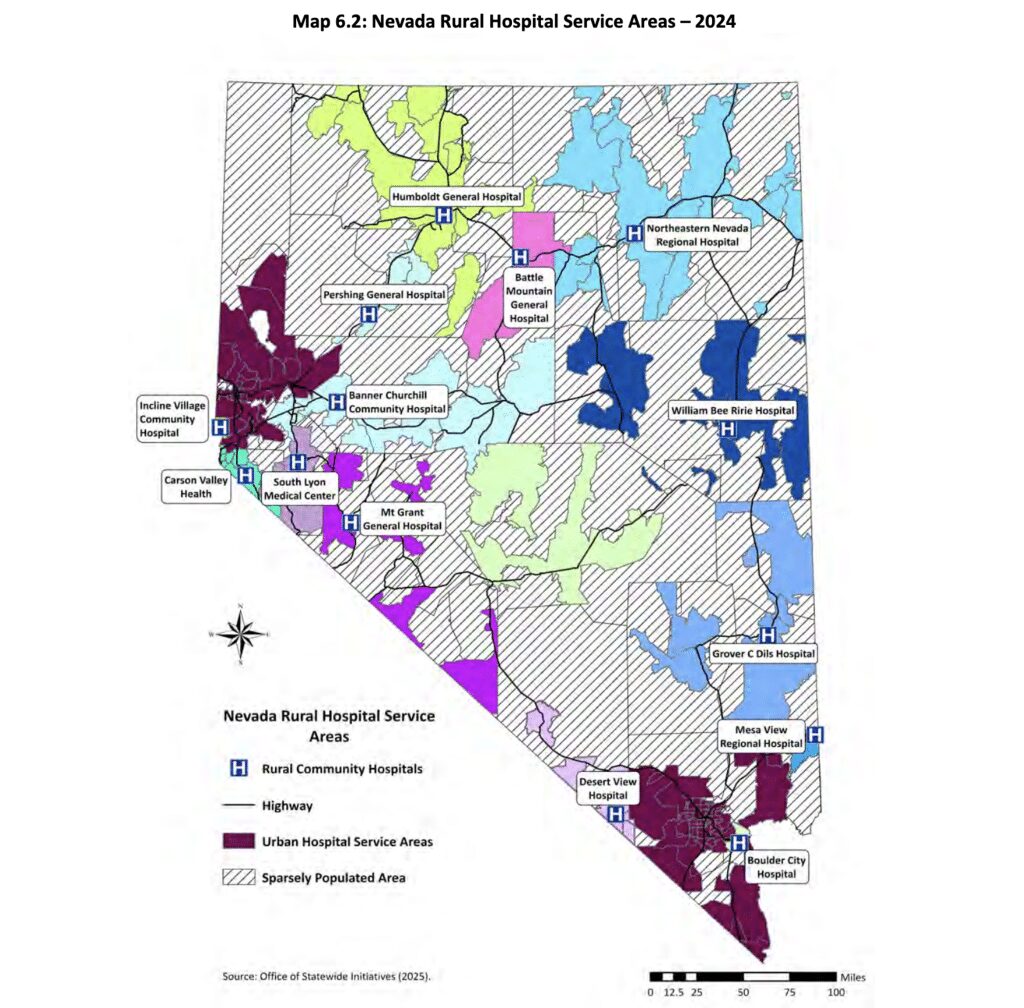
With providers overworked, patients are often left waiting months for appointments or forced to seek care outside their communities — many of which are in sparsely populated counties far from urban medical centers. According to the Nevada Office of Statewide Initiatives, "the average distance between acute care hospitals in rural Nevada and the next level of care or tertiary care hospital is 118 miles and the average distance to the nearest incorporated town is 46.3 miles." These long travel times and related costs contribute to poorer health outcomes and further widen health disparities.
Additionally, the number and geographic distribution of health care professionals and specialists adds to the strain. Overall, the number of licensed health professionals per 100,000 residents is lower in rural and frontier counties compared to urban centers, according to the Nevada Rural and Frontier Health Data Book-12th Edition, from January 2025, by the Office of Statewide Initiatives at UNR.
John Packham, associate dean for the Office of Statewide Initiatives at UNR, explains that this limited access, particularly to specialists, affects community health in profound ways. Residents must often leave their communities to receive care — sometimes relying on others for weekly transportation to Reno or Las Vegas, or in some cases, relocating permanently to urban areas to access the medical services they need.
Implications for Long COVID treatment in Northern Nevada
For Northern Nevada, standalone Long COVID clinics may not be the best fit given the state's realities. With much of the population spread across rural areas, specialized centers would likely be concentrated in urban hubs such as Reno — again leaving rural residents without access. At the same time, Nevada already faces severe shortages of primary care doctors and specialists, making it difficult to staff dedicated clinics without pulling resources from other critical services.
Training and retaining dedicated professionals is particularly challenging in rural regions. Packham notes that physicians and nurses who grow up and train in urban areas are often reluctant to relocate to frontier communities where travel distances are long and isolation is common.
"We have discovered that reaching out to middle and high school students in these communities, supporting them and sparking their interest in health careers makes them far more likely to return to practice in rural areas," he said.
Because diagnosing and reporting Long COVID remains difficult, it's unclear how many people in rural Nevada are affected. Packham says doctors are not seeing high volumes of Long COVID patients in these regions.
"I don't think there would be the demand for specialized clinics in rural areas. There is plenty of demand for primary care and hospital services — even long-term and nursing home care — but more specialized services like infectious diseases are less common. Less demand means a lower likelihood that there would be an available service there," Packham said.
Ongoing research and projects
While specialized Long COVID clinics might not be realistic for Nevada, several initiatives are bridging the gap. Programs such as Project ECHO, an initiative from the UNR School of Medicine, connect rural providers with specialists in Reno through telehealth — building local capacity without requiring patients to travel long distances.
The School of Medicine also hosts monthly rural outreach clinics in Yerington, Silver Springs and Fallon. These student-led clinics are free, offering primary care, lab work, immunizations and referrals.
"This is my favorite day of the month," said Pope, the rural health education coordinator. "Sometimes we diagnose simple issues that, without insurance, could cost a patient hundreds of dollars.
"Other cases are more serious — we once had an undocumented patient in Yerington diagnosed with a severe heart murmur that left him with only 6 to 8 months to live without surgery," she said. "With no insurance, he couldn't access care, but through legal counsel and the Mexican consulate, we helped him secure Medicaid. He got the surgery — and months later returned just to thank the students."
Globally, research continues to uncover why some people develop Long COVID and how best to treat it. These studies will be critical for developing better treatment strategies — and for helping patients like Crystal regain their health and their joy in food.
This article was supported in part by a National Association of Science Writers Investigative Reporting Grant.
Support Independent Elections Coverage and Journalism in Nevada
You’ve enjoyed unlimited access to our reporting because we’re committed to providing independent, accessible journalism for all Nevadans.
But sustaining this work — informing communities, holding leaders accountable, and strengthening civic life — depends on readers like you.
Nevada needs strong, independent journalism. Will you join us?
A gift of any amount helps keep our reporting free and accessible to everyone across our state and funds our elections coverage.
Choose an amount or learn more about membership