
I went to the emergency room this week


Before you ask — no, I did not have nor do I now have COVID-19.
My trip to the emergency room was of a more ordinary variety. While driving home from work on Tuesday, my chest felt a little tight and my heart felt like… well, like it was idling roughly. I'm not sure how better to describe it, but it felt exactly like a car feels when it has a failing spark plug, pounding erratically but not rapidly, only inside my chest.
This, by itself, was not entirely unusual. My heart has done this for a few minutes at a time out of nowhere for years. After talking to my friends about it and learning many of them felt the same thing from time to time, I just attributed it to "getting old" and added it to the short list of recurring annoyances my body produces, like my newfound need to wear glasses if I want to see clearly at a computer screen. Besides, I started exercising more over the past few years and noticed these heart stutters mostly went away. I told myself that it might be worth hitting the exercise bike before dinner.
This time, however, it didn't stop. Instead, after I got home and ate some dinner (I passed on the exercise bike), it got worse. When I started to get a little dizzy, I decided it was time to collect some data so I better understood what was going on.
When COVID-19 first appeared, like a lot of Americans I did some impulse shopping for home health equipment. One of the items I picked up was a personal electrocardiogram, or EKG, device which wirelessly communicates with my phone. Normally, when everything is working as it should, it produces an EKG which looks something like this:

This, according to my phone's EKG app (I'm an IT manager, not a doctor, so please take this all with a grain of salt) is "normal sinus rhythm". Just as a properly running car coordinates the firing of its spark plugs with the motion of the pistons in your engine (unless you're driving an electric car or an older Mazda), your body times the triggering of each heart muscle contraction with the pumping action created by the rest of your heart's muscles. When current is flowing correctly from the brain, through the nervous system, into the sinoatrial (the "sinus" in "normal sinus rhythm") node, then finally to the heart's muscles, it produces that trademark "thuh-THUMP" heartbeat pattern we all know and heart emoji react to. The above EKG reflects that trademark pattern by showing a sharp wave, followed by a longer wave, followed by a regular interval until the next sharp wave.
That evening, however, my EKG looked like this:
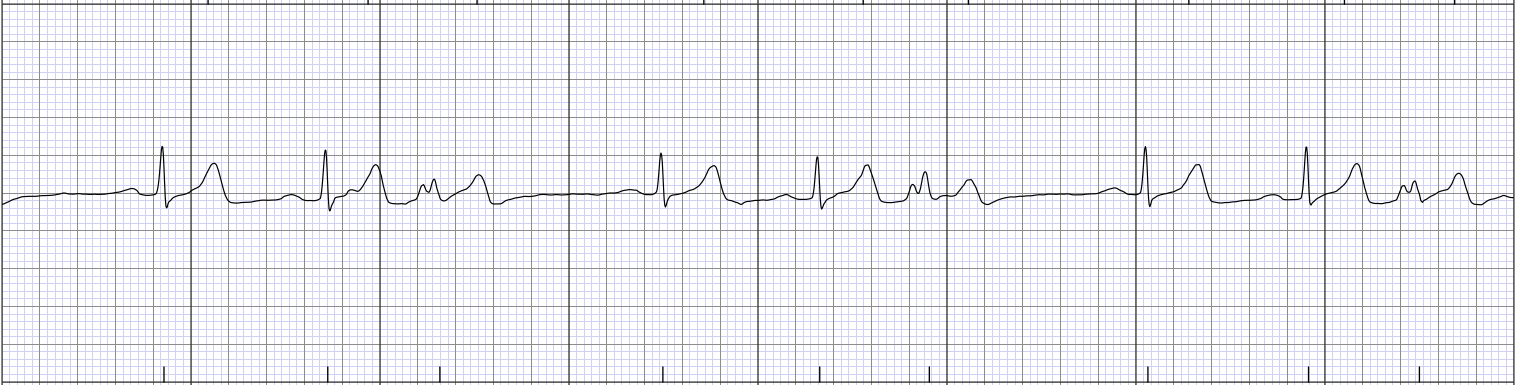
My heart wasn't going "thuh-THUMP". It was going "thuh-THUMP thuh-THUMPthumpthump". This, according to my phone's EKG app, wasn't "normal sinus rhythm". Instead, it was "unclassified". Now, speaking from personal experience, it's incredibly reassuring when your body does such a lackluster job of performing a routine yet vital bodily function you ordinarily don't think about that it completely baffles an internet-connected medical application.
Filled with the sort of confidence an "unclassified" heartbeat pattern gives a man, I decided I collected enough data to start a conversation — first with my fianceé, who was growing increasingly concerned over my sudden fascination with collecting personal medical data about my heartbeat (especially after she listened to my chest), then subsequently with a doctor.
Still, it was late and I didn't think I was dying, at least not right away. Well, I was pretty sure I wasn't, anyway. More accurately, my level of surety in not experiencing immediate mortality in that specific moment was, shall we say, unclassified. So I decided to throw another phone application at the problem — this time a telemedicine application. Fifteen minutes later, I was connected to a videoconference with a doctor who, after I described my symptoms, told me I needed to get a real EKG from a real doctor with real equipment.
Here in the Reno-Sparks area, when you need an EKG at nine o'clock at night, there's really only one place to get one — an emergency room. Under the best of American circumstances, that's not exactly ideal, especially when your medical insurance politely but firmly reminds you each year that, to keep their costs under control, they will creatively apply non-Euclidean hypergeometries against your finances every time you make eye contact with one.
We are not, however, living in Panglossia Americana.
No, my heart decided to practice its paradiddles in the middle of a pandemic that's pushing emergency room capacity towards the ragged edge. As I write this, according to the Reno Gazette-Journal, the hospital closest to my home, Northern Nevada Medical Center, has 105.5 percent of its inpatient beds in use (I'm guessing a few of their patients are stacked on top of each other like cordwood). Meanwhile, Renown, the largest hospital in the area, is currently at 92.3 percent of inpatient capacity. Roughly a quarter of the patients in those beds tested positive for COVID-19.
So my fianceé and I put on our finest N95 masks and went to the Renown emergency room and field-tested our triple-espresso vaccinations.
***
The good and bad news about COVID-19 vaccines is they're a lot like the antivirus products I have to deal with at work — they work far more often than not so long as you continuously apply regular updates. According to the CDC, vaccine effectiveness for mRNA vaccines, like Pfizer or Moderna, against emergency room or urgent care visits triggered by the Omicron variant is 82 percent, provided you recently received a third shot. Unfortunately, vaccine effectiveness is considerably worse if you only received two shots of an mRNA vaccine, especially if that last shot was a while ago. According to the same study, vaccine effectiveness against Omicron drops to 38 percent for patients last vaccinated against COVID-19 over 180 days ago.
Trouble is, like the antivirus products I have to deal with at work, mRNA vaccines can leave you feeling a little slow sometimes. Don't get me wrong, they beat the alternative — if I suggested to my chief information security officer that our office network should pursue "herd immunity" against ransomware attacks, I'd be out of a job and rightly so, especially if I followed the same heuristic of one of the authors of the Great Barrington Declaration — a piece of early pandemic esoterica which assumed (falsely, it sadly turns out in hindsight) that past exposure to COVID-19 leads to future immunity, so the way out of the pandemic would be to just let the virus spread as fast as possible — and knowingly plugged ransomware-infected media into my work computer to create "constant reinfection". Ransomware attacks, like severe COVID-19 infections, are incredibly painful and destructive to everyone involved and should be avoided as much as practically possible.
Even so, it would be nice if we had a COVID-19 vaccine that was more like our childhood vaccines. Of course, it would be even nicer if we didn't have to deal with a COVID-19 pandemic or office-wide ransomware infections at all.
Alas.
***
The first thing I noticed once we reached the emergency room was that my fianceé could join me in the waiting room. The last time either of us had been anywhere near an emergency room, patients had to enter the waiting room on their own. This, however, turned out to be a short-lived pandemic mitigation measure, one which was rolled back in June 2020 and relaxed further in May 2021.
The second thing I noticed was the efficiency of the triage process. The hospital checked me in, had me sign a pile of paperwork (more on that in a minute), took an EKG, explained the results of the EKG (I was experiencing premature ventricular contractions and bradycardia), and took some blood samples for some subsequent lab work, all before my fianceé was even done parking the car after dropping me off at the hospital.
With those pleasant surprises out of the way, things became progressively worse after that.
Part of the problem was the triage process, which is designed to identify which patients have the most urgent medical needs. The goal for an emergency room is to treat those who need urgent treatment as fast as possible — which, I quickly grew to realize, did not mean me. Several of the other patients in the waiting room were clearly in more immediate distress. One woman sitting in front of me, for example, alternated between sleeping and coughing hard enough to turn purple, all with her mask around her neck.
I'm not sure how long she waited before I sat across from her in the waiting room, but she waited at least three more hours before she was ushered out of the waiting room. When I saw her finally get admitted past the waiting room, I suspected, given that I wasn't turning purple nor hacking up a lung, that I'd be waiting a while longer. I was right — my fianceé and I would ultimately continue waiting for another four hours.
During those seven hours in the waiting room, we both did some light reading. She read everything she could find about bradycardia, premature ventricular contractions, and heart arrhythmias more generally. I, meanwhile, was reading Bryan Burrough's Days of Rage, a historical recount of the pathetic and Sisyphean attempts to start an armed revolution certain radical leftists tried to put together during the 1970s, all while trying to distract myself from the reality of my medical situation, our surroundings, and the length of the wait.
I thought about leaving (my fianceé, after a cursory internet search, concluded doing so would likely lead my health insurance provider to refuse to pay for the trip). I thought about the pile of paperwork I signed which told me I could expect a bill from the hospital, a bill from the lab, a bill from my doctor, a bill from the janitorial services company cleaning the bathrooms, a bill from the manufacturer of the chair I was sitting in, and a bill from any other semi-independent corporate entity Renown Health could claim was within ten parsecs of my medical chart (incidentally, Renown Health is currently suing the federal government to relax some of the restrictions against third-party billing the hospital reluctantly works under). I thought about my chest, which was admittedly feeling better.
Meanwhile, the number of patients entering the emergency room steadily decreased and the chairs surrounding us steadily emptied. By 5 o'clock in the morning, hardly anyone was left in the waiting room with us. Finally, it was my turn to get escorted to a hospital bed.
Two hours later, the visit was complete and we went home.
The doctor was clearly tired, with dark rings around his eyes, yet still somehow friendly and professional. Looking back, there wasn't a single surly or difficult nurse in the bunch — somehow, despite obvious signs of strain and fatigue, each and every hospital employee (or "subcontractor", for out-of-network insurance billing purposes) was unfailingly polite, kind and supportive.
Whatever it is that's wrong with the American health care system, it's not with the people working within it.
***
Since visiting an emergency room is a lot like visiting a DMV — it's something nobody wants to do, we always wait longer than we'd like, there's always a near-inscrutable pile of paperwork involved — it's common to want to vent and use the experience to paint the rest of our healthcare system with a broad brush.
With that in mind, in exchange for an EKG, a few blood tests, a COVID-19 PCR test (I tested negative), a seven hour wait in a waiting room, one x-ray, two hours on a hospital bed, and approximately 15 minutes with a doctor, my insurance company is probably going to receive a bill from the hospital that would exceed the price of a new car. My insurance company, in turn, will subtract my deductible and my "coinsurance" (a delightfully Orwellian bit of doublespeak meant to suggest I am acting as my own insurance provider when my insurance company refuses to pay 20 percent of my ER bill) and cut a check to the hospital for the difference. The hospital will then, finally, send me a bill for whatever's left.
I have no idea what that number will turn out to be. It could be a few hundred dollars. It could be a few thousand dollars. It could be tens of thousands of dollars.
I can't tell you whether the doctor I saw in the emergency room is in my insurance company's network of providers or not. I can't tell you whether the lab used by the emergency room to determine my blood had a slightly lower concentration of neutrophils and a slightly higher concentration of lymphocytes than is considered within the "standard range" is in my insurance company's network of providers or not. I can tell you Renown is "in network" (Saint Mary's and its considerably less crowded inpatient facility is not), but I couldn't begin to guess what my insurance company and Renown have mutually agreed is a fair rate for hospital services.
The worst part is I can't even begin to guess what's wrong, if anything, with my heart. I have a follow-up appointment with a cardiologist next week to hopefully start finding that out. It might be nothing. It might be something. Who knows? Either way, my insurance company and I will probably pay Renown enough to put a student through a semester at a nice, leafy private university somewhere. Maybe two students, if we're really lucky.
All of that, however, is tomorrow's problem.
For now, I will at least be thankful that, in the middle of a pandemic, there was a doctor available to see me in the middle of the night, I didn't have to sit in the waiting room alone, and I didn't need much more than that. All of that is not nothing — and it's more than I was expecting.
David Colborne ran for office twice and served on the executive committees for his state and county Libertarian Party chapters. He is now an IT manager, a registered non-partisan voter, the father of two sons, and a weekly opinion columnist for The Nevada Independent. You can follow him on Twitter @DavidColborne or email him at [email protected].
Support Independent Elections Coverage and Journalism in Nevada
You’ve enjoyed unlimited access to our reporting because we’re committed to providing independent, accessible journalism for all Nevadans.
But sustaining this work — informing communities, holding leaders accountable, and strengthening civic life — depends on readers like you.
Nevada needs strong, independent journalism. Will you join us?
A gift of any amount helps keep our reporting free and accessible to everyone across our state and funds our elections coverage.
Choose an amount or learn more about membership